Statins Will Kill You
This article is a talk I gave at the 34th Annual Meeting of Doctors for Disaster Preparedness in Omaha last week. Its director, Jane Orient, M.D., asked me to address the subjects of statins, nutritional supplements, stem cells, and hyperbaric oxygen for combating heart disease. The text includes some of the slides I used for this talk.
Heart Disease
My father was born and raised on a farm in Nebraska and attended medical school at the University of Nebraska, Class of 1938. He died from a stroke, at age 97. Heart disease, however, remains the leading cause of death in this country, which ends a person’s life at a much younger age. Cancer is next, close behind heart disease, which causes 40 percent of all U.S. deaths.
A systematic review published last month in the British Medical Journal confirms the finding that people with a high cholesterol live longer. [1]
How Statin Drugs Kill You One Cell at a Time
The book How Statin Drugs Really Lower Cholesterol and Kill You One Cell at a Time by James Joseph and Hannah Joseph, M.D. reveal in chilling detail how statins harm people. A reviewer of this book writes:
“Many practicing physicians have a healthy understanding of the current level of corruption and collusion among big pharmaceutical companies, governmental agencies such as the NIH and FDA, and major medical associations such as the American Heart Association, but the reader of this book will come away with the disturbing conclusion that it is even worse than imagined. Statins may be the perfect and most insidious human toxin in that adverse effects are often delayed by years and come about gradually. Further, statins frequently impair mental function to such a degree that by the time patients are in real trouble, they may lack the mental facilities to recognize the cause.”
Adverse Effects of Statins
Statins target skeletal muscle and brain cells. Myopathy, manifested by muscle aches and pains, weakness and instability is the most common adverse effect of statins. The severist manifestation of statin-induced muscle damage is rhabdomyolysis, which carries a 10 percent mortality rate. Fragments of ruptured muscle block renal tubules and cause kidney failure.
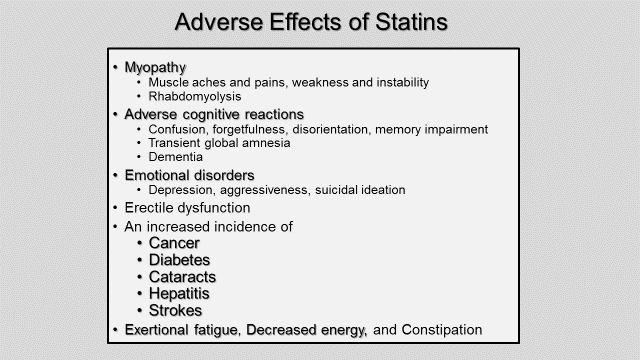
A number of statin trials report a statistically significant increased incidence of cancer, cataracts, hepatitis and strokes associated with taking statins.
Approximately 8 percent of people who take statins get diabetes, compared with 2 percent in the placebo group. Investigators will say that there is a 6 percent chance of getting diabetes from taking statins. They will report deleterious effects in terms of real, absolute risk, thus minimizing their magnitude. You will not see statin-trial investigators reporting that there is a 75 percent increased risk of getting diabetes from taking statins, its relative risk (where 8 – 2 = 6 and 6 divided by 8 equals 75 percent).
The FDA issued new safety information on statins in 2014, saying “a small increased risk of raised blood sugar levels and the development of type 2 diabetes have been reported with the use of statins.” The FDA now requires drug companies to add this information in their package insert with the drug. After issuing this conclusion, over the next 6 months, attorneys filed more than 1,000 lawsuits against Pfizer for (4,000) women claiming that Lipitor gave them diabetes.
Adverse cognitive reactions from taking statins include confusion, forgetfulness, disorientation, memory impairment, transient global amnesia, and dementia.
Can Statins Actually Cause Heart Disease?
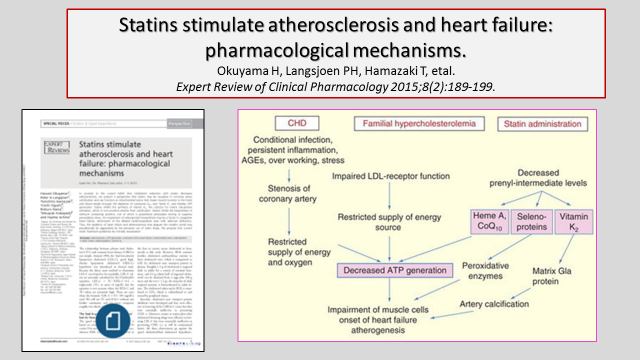
Unfortunately, as the study cited above shows, statins may well promote both types of heart disease, atherosclerosis and heart failure. Arterial calcification fosters atherosclerosis but a special protein, matrix Gla protein removes calcium in arteries. Vitamin D turns on the gene that makes matrix Gla protein, and vitamin K2 is required to activate it. But statins block the conversion of vitamin K1 to K2. With statins also blocking CoQ10 and heme A synthesis, generation of ATP in heart muscle cells decreases, leading to heart failure. This study, published last year in Expert Review of Clinical Pharmacology and citing 56 scientific references, shows the mechanisms by which statins stimulate atherosclerosis and heart failure.
Patients Beware
I worked with cardiologists during my 40-year career as one of their heart surgeons. Given so much damning evidence against statins, how can they keep on prescribing them? Three reasons come to mind. First, cardiologists are busy and don’t have the time or inclination to independently investigate things and read a lot of medical journals (like Expert Review of Clinical Pharmacology). They accept what their medical societies and statin-selling drug reps tell them about statins. Second, not wanting to be accused of practicing what health authorities deem “low-quality” medicine, cardiologists dutifully prescribe statins following medical society/government certified cholesterol-lowering guidelines. Third, like many professionals, mainstream cardiologists suffer from a healthy dose of confirmation bias, where they filter out and ignore evidence that doesn’t coincide with their preconceived notions and beliefs, especially with regard to statins.
The Current State of Medical Science
As we see with statins, medical science today is in a sorry state. Dr. Marcia Angell, former editor-in-chief of the New England Journal of Medicine writes:
“It is simply no longer possible to believe much of the clinical research that is published, or to rely on the judgment of trusted physicians or authoritative medical guidelines. I take no pleasure in this conclusion, which I reached slowly and reluctantly over my two decades as an editor of the New England Journal of Medicine.”
Dr. Richard Horton, current editor-in-chief of the Lancet agrees:
“The case against science is straightforward: much of the scientific literature, perhaps half, may simply be untrue. Afflicted by studies with small sample sizes, tiny effects, invalid exploratory analyses, and flagrant conflicts of interest, together with an obsession for pursuing fashionable trends of dubious importance, science has taken a turn towards darkness.”
PCSK9 Inhibitors
To make matters even worse, the FDA has approved a cholesterol-lowering drug that you inject twice a month costing $14,000 a year ($583 a shot). Working by a different mechanism a PCSK9 inhibitor lowers LDL cholesterol even more than the most potent statin. Amgen makes one called Repatha. Trials gaining FDA approval for the safety and efficacy of this injectable drug lasted only 12- to 52-weeks, much too short a time to uncover late-developing cerebral ill-effects like confusion, forgetfulness, disorientation, memory impairment, and dementia—things that PCSK9 inhibitors, since they severely lower cholesterol, might well cause.
Russell Ross and Inflammation
If not cholesterol, what causes atherosclerosis? The late Russell Ross, professor of pathology at the University of Washington, discovered the cause: Atherosclerosis is an inflammatory disease. It is initiated by endothelial dysfunction, with or without actual injury. Macrophages and T lymphocytes mediate it, and smooth muscle cells play an integral role.
Russell demonstrated that atherosclerosis is a chronic inflammatory and fibroproliferative process that is
fundamentally no different from that seen in cirrhosis, rheumatoid arthritis, and chronic pancreatitis. I worked Dr. Ross and attended cardiology conferences him. The New England Journal of Medicine published his landmark paper on atherosclerosis being an inflammatory disease just a few months before he died, from cancer.
Inflammation and NF-kB
Inflammation plays an important role in other chronic diseases like diabetes, cancer, and Alzheimer’s disease.
Nuclear factor kappa B, NF-kB, is a key protein transcription factor that promotes inflammation. Statins’ small 1 percent benefit come from their anti-inflammatory effects, suppressing NF-kB. Two non-prescription nutraceuticals, curcumin, and resveratrol, have the same NF-kB suppressing anti-inflammatory action, without having any side effects.
Things that Foster Inflammatory CAD
Things that foster inflammatory atherosclerotic heart disease starts with a bad diet: consuming too many omega-6 vegetable oils, eating trans fats, too many carbohydrates, and not enough saturated fats. See my LewRockwell.com article “Enjoy Saturated Fats, They’re Good for You!” for more on this subject. Other things that foster inflammatory coronary artery disease include deficiencies in various vitamins and minerals, having diabetes, abdominal obesity, hypertension, smoking, stress, and a family history of heart disease. Another cause, it turns out, is a bacterial infection. Like in the stomach, it is becoming increasingly evident that the bacteria Helicobacter pylori can also cause coronary artery disease.

Nutritional Supplements
From my research on this subject, these are 14 supplements that may help prevent and, if already present combat heart disease—along with taking a multivitamin pill:
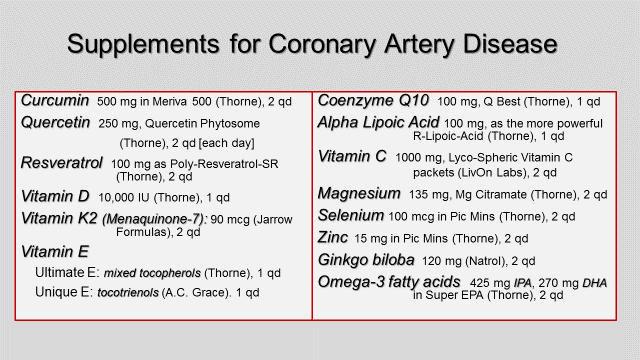
I provide short descriptions of each of these nutritional supplements—their respective mechanisms of actions, doses, where I get them, and their costs—in my April 15, 2015, LewRockwell.com article, “Supplements for Coronary Artery Disease.” The cost of taking all of them each day is not much more than what a 20 mg tablet of Crestor costs.
This slide offers a summary view of their various mechanisms of action:

Evidence of Effectiveness
There is evidence that a nutritional supplement program like the one proposed here can halt the progression of coronary atherosclerosis and reduce coronary calcification. In one study, 55 patients with positive coronary calcium scans, documented by ultrafast computed tomography, were put on a nutritional supplement program that included 6 of the ones on my list plus a multivitamin tablet. One year later investigators repeated the coronary calcium scan. The calcium score in these 55 patients had decreased by an average of 11 percent, decreasing the most in patients with the early coronary disease. In one patient, calcium in the right coronary artery and left anterior descending coronary artery was greatly reduced. [2] (Slide available on request.)
In another randomized trial of people with moderate to severe heart failure, a significantly higher percentage of patients taking 300 mg a day of coenzyme Q10 remained free of major adverse cardiovascular events compared with patients taking a placebo. A secondary outcome that the study tracked was death from any cause, and people taking coenzyme Q10 had an overall statistically higher survival rate than those taking a placebo. [3] (I also can send you a slide showing these graphs.) Unlike heart drugs that physicians prescribe, “over-the-counter’ coenzyme Q10 has no side effects.
A long-term, large-scale randomized trial of people taking these nutritional supplements compared with a group taking a statin and aspirin, along with a control group on a placebo would greatly help to verify their value. The federal government currently funds 51 percent of the 20,000 interventional trials that researchers are conducting. Universities, foundations, and other organizations sponsors 25 percent; and pharmaceutical companies, 24 percent. [4] One can be sure that drug companies, the government, and politically correct universities will never fund a nonpatentable study like this.
Seed Nutrition
A physician in Seattle, Brad Weeks, M.D., a fellow Dartmouth alumnus, told me about seed supplements. These cold-pressed, liquefied seeds taste like pomegranate juice. The 2 oz., a 35-calorie packet of Rain Soul contains black cumin, chardonnay grape, and black raspberry seeds. The 1 oz., 15-calorie Rain Core has the 10 seeds shown in the slide below. They contain phospholipids; vitamins, and minerals; are rich in the essential Omega-6 linoleic and Omega-3 linolenic acids; are high in natural anti-oxidants, and they contain various anti-inflammatory agents. (An extract from black cumin seeds, thymoquinone, has been shown to kill colorectal, prostate, and breast cancer cells.)

Rain Soul
Studies show there are 20-fold more nutrients concentrated in a seed compared to the rest of the plant. One packet of Rain Soul contains the equivalent of 8-10 servings of both fruit and vegetables and 2-3 servings of healthy oils. Given their anti-inflammatory and anti-oxidant components, drinking liquefied seeds might well turn out to be a good way to help prevent and combat heart disease.

People with all different kinds of chronic pain also report surprising relief drinking these seeds, along with applying them topically to a painful area on the body. My wife Linda and I have been taking two packets each of the Soul and Core seeds every day now for six months. The pain she has suffered in her hands and knee from osteoarthritis is much reduced. For me, I turn age 76 next month but feel like I’m 56.
Topically applying the Soul oil cleared up a persisting skin disorder my wife had on her forearm.

After several weeks rubbing these liquefied seeds on it, this inflammatory lesion completely resolved and has not come back. Linda and I have become so impressed with these seed oils that we have signed on with Rain International, the company that makes them, as seed nutrition affiliates. I don’t know if they can prevent heart disease, but it surely looks like they are good for one’s health, judging from our own experience and many testimonials on them. For anyone who might be interested in trying them, visit our website wellnesswithseeds.com or talk to Linda or me at the phone number below:

Stem cells
These cells are distinguished by the fact that they can replicate themselves; and they are undifferentiated, thus capable of giving rise to specialized cells. They can morph into many different cell types, including new heart muscle cells, cardiomyocytes.
Heart Response to Injury
The response to the death of muscle in a heart can take two paths: regeneration and restoration of function or fibrosis and contractile dysfunction. In humans following a heart attack, a myocardial infarction that kills heart muscle, the dead muscle is replaced with scar tissue, with resulting contractile dysfunction. But, remarkably, the hearts in neonatal mice less than a week old, newts, and adult zebrafish respond to heart injury and cell death by regenerating new muscle and accompanying blood vessels. A zebrafish can have 20% of its heart wrecked and still completely restore it back to normal.
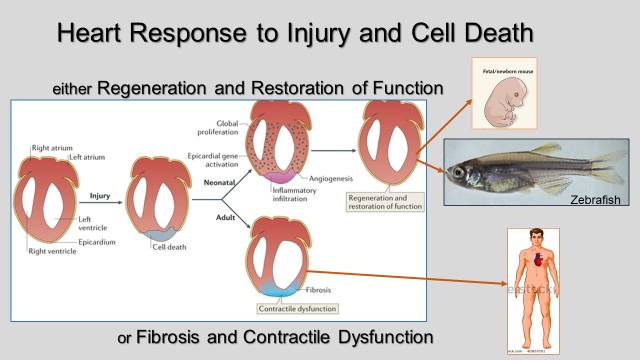
So why can’t our hearts be made to function like the one zebrafish have and regenerate itself?
Cardiomyocyte Renewal
Until fairly recently, it has been that heart muscle cells are postmitotic, meaning they don’t divide and have to function all through the entire lifespan of an individual without being replaced by any new ones. Atmospheric nuclear weapon tests first provided a means to refute this idea.
Before 1955 when atmospheric nuclear bomb tests began, the isotope carbon-14, with a half-life of 5,730 years, existed in the atmosphere in a low and stable concentration. It combines with oxygen to form carbon dioxide, which plants consume and then humans eat (along with eating animals that also eat plants). It’s like how Woody Allen views to nature, as an enormous restaurant where everybody eats each other. This isotope of carbon gets incorporated into our cells. The concentration of carbon-14 in the atmosphere rose substantially and peaked in 1963 when the Nuclear Test Ban Treaty was adopted, and it then dropped back toward its baseline level. In people born before 1955, measurement of carbon-14 concentrations in their cardiomyocyte DNA and proteins specific to those cells, troponins, shows that some of their heart muscle cells were formed after they were born and are relatively new. Cardiomyocyte turnover does occur in humans, replacing the ones people were born with when atmospheric carbon-14 concentrations were low with new muscle cells that have a high level of carbon-14.
So, muscle cells in the human heart, like in zebrafish, do in fact renew and replace themselves, to some degree, with new muscle cells. Investigators who first discovered this using carbon-14 as a marker calculate that humans renew their cardiomyocytes at a rate of ~1 percent per year at age 25, dropping as one gets older. By age 50, they calculate, approximately 45 percent of a person’s heart muscle cells have been replaced with new ones. [5]
Another group more recently employing different techniques have concluded that the annual turnover of human cardiomyocytes is much higher, especially in women, and that myocyte regeneration increases with age. These investigators calculate that all the heart muscle cells present at birth completely turnover by the time one becomes a young adult, have completely turned over once again in a middle-aged person, and have completely turned over yet a third time in the senescent heart. [6]
Types of Stem Cells
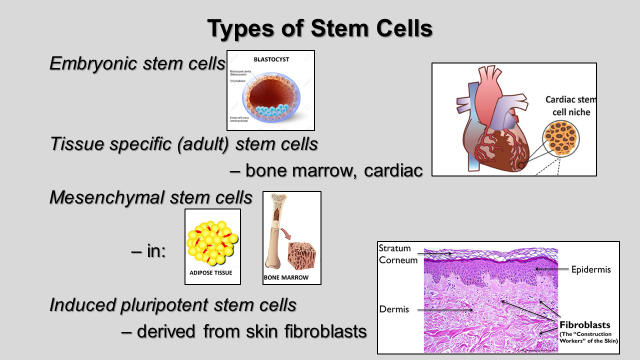
There are four basic types of stem cells: Technicians extract embryonic stem cells from an in vitro fertilized, 0.1 to .2 mm human embryo that has reached the 5-day-old, 200 to 300-cell blastocyst stage. These cells have the capacity to differentiate into all the different types of cells that are in the 3 germ layers: endoderm, mesoderm, and ectoderm. Although the best kind of stem cell, ethical concerns prevent using human embryonic stem cells as a treatment modality in patients.
The heart has its own resident adult cardiac stem cells that congregate in niches in the apex of the left ventricle and right and left atria. They can turn themselves into new cardiomyocytes, vascular smooth muscle, and endothelial cells. Mesenchymal stem cells are multipotent stromal cells that can differentiate into a variety of different cells, and in the laboratory, specialists can expand and reprogram them to become heart muscle cells. They make up one in every thousand cells in the bone marrow. And then there are induced pluripotent stem cells. Skin fibroblasts obtained from a skin biopsy are one kind. Laboratory technicians genetically reprogram and engineer them to behave like an embryonic stem cell with all its potential.
Stem Cell Clinical Trials
The journal Nature, in its weekly May 1, 2014, issue, reported on doubts arising over heart stem-cell therapy. The British Medical Journal had just published a systematic review of 49 supposedly randomized trials studying the effect of bone marrow stem cells on improving heart function in people with heart failure. These trials measured the heart’s ejection fraction, the percent of blood the left ventricle pumps out with each beat, which is normally 66%. Apropos of what Drs. Angell and Horton say about the state of medical science, investigators found that 44 of these 49 trials were rife with discrepancies. They scrutinized the design of each study, its methods, baseline characteristics, tables, figures, and reported results, looking for instances where two or more facts or statements could not both be true since they were logically or mathematically incompatible. Five trials with more than 30 discrepancies reported the best results, showing an average improvement in ejection fraction of 7.7 percent. Just 5 of the 49 trails had no discrepancies. These carefully done, honest trials showed a slight decrease in ejection fraction in the people treated with stem cells. [7]
Trials using mesenchymal or adult cardiac stem cells so far have shown disappointing, negligible effects. SCIPIO (the acronym for “cardiac stem cell infusion in patients with ischemic cardiomyopathy”) was the first randomized trial using adult cardiac stem cells. Investigators enrolled 33 people who had an average ejection fraction of 27%, in the study. Each person first underwent coronary artery bypass surgery, the operation I taught and performed. The surgeon removes part of the right atrial appendage. Technicians extract stem cells residing in the biopsy, grow them in test tubes for 4 months and expand their number to a million cells. In 20 patients these person-specific, autologous cultured cells are injected back into the heart through a catheter placed in the coronary artery supplying damaged muscle, with 13 patients left alone serving as a control. A preliminary report looked promising, but officials at one of the universities participating in the study (Harvard) retracted it when faculty readers found what they termed “scientific irregularities” in the study, which to date remain undefined.
In all trials so far the vast majority of the transmitted stem cells die within a week.
Proposed Mechanisms of Cell Therapy for Heart Regeneration
Three proposed ways for carrying out stem cell therapy for heart failure are: use cardiac stem cells obtained from the septal wall of the person’s heart, mesenchymal stem cells harvested from one’s bone marrow, or to use induced pluripotent stem cells made from another person’s skin-biopsy-obtained fibroblasts. Each kind is
expanded in the laboratory, in vitro, and with pluripotent cells engineered to become new heart muscle cells. They are delivered by a catheter a cardiologist inserts through the skin into an artery in the wrist or groin and then threads it up to the heart, injecting the cells either in the coronary artery supplying damaged muscle, or, placing the catheter inside the left ventricle, directly into the affected muscle, into its inner, endocardial side.
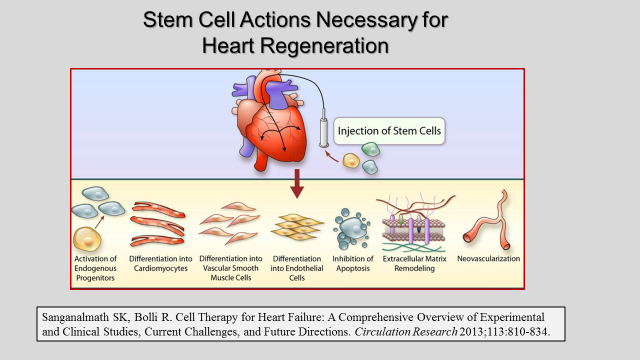
Stem Cell Actions Necessary for Heart Regeneration
For stem cells to successfully replace failing, injured, or dead heart muscle, they have to do a lot of things, in addition to becoming new muscle. They also have to differentiate into vascular smooth muscle cells and endothelial cells, promote neovascularization, remodel the extracellular matrix, inhibit apoptosis (cell death), provide paracrine signaling (localized hormone-like chemical signals) to adjacent cells, and establish appropriate electrical connections to synchronously contract with other heart muscle cells. Plus, they have to be able to repair adverse cardiac remodeling and reduce hypertrophy.
Work on stem cells has a way to go before they will be ready for clinical use, especially ones available “off the shelf” that do not require a biopsy and time to process them before they can be used. Already processed, induced pluripotent stem cells from other people, allogenic ones, which work well and have no immunologic or other side effects would fit the bill.
Heart repair with stem cells holds enormous promise. But it will probably be another ten years before they are ready-to-go on the shelf. Nevertheless, they should be ready in time to treat all the people who develop heart failure from taking statins.
Hyperbaric Oxygen
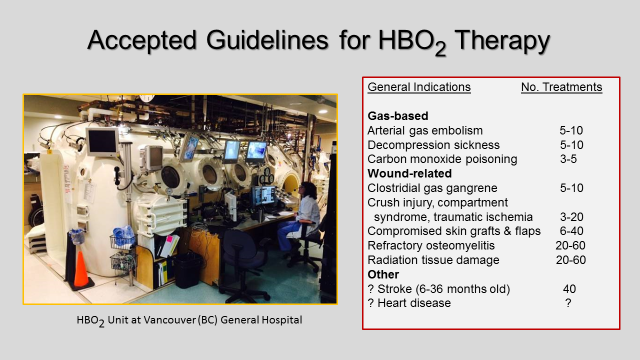
What about hyperbaric oxygen treatments? A typical HBO2 treatment is to breathe 100 percent oxygen at 1½ to 3 times increased atmospheric pressure for up to 1 to 2 hours
Indications
Hyperbaric oxygen therapy is either gas-based or wound-related, for the conditions listed below, but not, as things presently stand, for cardiovascular problems. Doctors that run this multiperson HBO2 unit in Vancouver BC are testing to see if it works for strokes. They are enrolling 140 people who have had a stroke in the past 6 to 36 months and will have them undergo 40 treatments to see if they improve cognitive skills and depression.
Portable HBOT
Now, for $20,000, you can have your own portable hyperbaric oxygen chamber.

NFL Players with Portable Hyperbaric Oxygen Chambers
More than 150 active and retired NFL players, which include Bret Favre, Donovan McNabb, Michael Vick, and several Seattle Seahawks players each have their own portable hyperbaric oxygen chamber. New York Giants running back Rashad Jennings says he spends 7 to 20 hours a week in his.
HBOT for Diastolic Heart failure
Studies to date using hyperbaric oxygen therapy for treating unstable angina and heart attacks—acute coronary syndrome—show no significant benefit. There is some evidence, however, that hyperbaric oxygen therapy improves heart function in diabetic patients. There are two kinds of heart failure: systolic, where weakened heart muscle doesn’t squeeze well. Stem cells hold promise for treating this kind of heart failure.
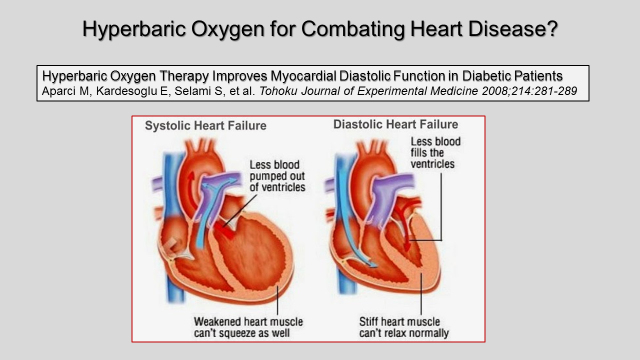
Some 30 percent of people with heart failure have a diastolic kind of failure, where stiff heart muscle can’t relax properly so less blood gets into the ventricle to be pumped out. In the study shown here, 30 diabetics with diastolic heart failure underwent 10 hyperbaric oxygen treatments over a 2-week period. After the treatments tests showed that their heart muscle could relax better, enabling the ventricle to fill up with more blood, thereby improving the ejection fraction and cardiac output.
HBOT’s Effect on Water
It is well understood how hyperbaric oxygen treatment works for gas-based conditions but not for wound-related treatments.
A study done by my colleague and friend Dr. Gerald Pollack, professor of bioengineering at the University of Washington and published in the journal Undersea and Hyperbaric Medicine shows what hyperbaric oxygen does to water.

Studies in his lab document that hyperbaric pressure and oxygen, each alone, builds up the fourth phase of water discovered by Dr. Pollack and termed interfacial exclusion zone (EZ) water. EZ water is a semi-liquid, gel-like, structured form of water, a fourth phase that coats proteins and cells, enabling them to fold and function properly. A molecule of EZ water is H3O2, having two oxygens, unlike bulk water (H2O) with one. Exclusion zone water stores energy, the only phase of water which does this. With its negative charge, EZ water supplies energy to the body that drives chemical reactions, capillary blood flow, and cellular work.
High concentrations of oxygen in the blood expands this phase of water, as does hyperbaric pressure alone. Like with ice, EZ water, with its stacked, honeycomb, hexagonal structure remains in place and is slow to dissipate. Hyperbaric oxygen’s effect on expanding this fourth phase of water may best explain how this short-lived treatment can exert a persistent and lasting beneficial effect on wound healing.
There are 12 Nobel Laureates at the University of Washington, and I predict that the next faculty member at this university to be awarded a Nobel Prize will be Dr. Pollack for his discovery of this fourth phase of water and his showing that this phase stores energy and obtains it from sunlight.
Oxygen Therapy Alone
Oxygen all by itself expands EZ water, with atmospheric pressure left alone, unchanged. A company named LiveO2 makes a generator that concentrates oxygen by filtering out and removing nitrogen from the air. The processed high-oxygen air is transferred and stored in a reservoir, a large bag, from which one breathes while exercising.
Like with stem cells, over the next 10 years, a lot more will be learned about breathing increased concentrations of oxygen, with or without hyperbaric pressure, to improve health and treat various conditions.
Conclusion
In closing, before heading back home to Leavenworth, Washington I urge you to do this: Refuse to take statins. Consider taking nutritional supplements to help protect against acquiring heart disease, or if already present, to combat it. Stem cells, hyperbaric oxygen, and oxygen treatment alone lie in the wings awaiting further research.
And for those of you who like to keep abreast of important new scientific discoveries, read Dr. Pollack’s (very readable) book The Fourth Phase of Water.
(Doctors for Disaster Preparedness, DDP, will be releasing a video of this talk on YouTube with all of its 57 slides—23 of them are shown here. Also, a video of my talk “Enjoy Saturated Fats, They’re Good for You,” given at an earlier DDP meeting, which includes a clip from Woody Allen’s movie Sleeper, is available on YouTube HERE.)
References
1 – Ravnskov U, Diamond DM, Hana R, et al. Lack of an association or an inverse association between low-density lipoprotein cholesterol and mortality in the elderly: a systematic review. British Medical Journal Open 2016;6:e010401 doi:10.1136/bmjopen-2015-010401.
2 – Matthias R, Niedzwiecki A. Nutritional Supplement Program Halts Progression of Early Coronary Atherosclerosis Documented by Ultrafast Computed Tomography Journal of Applied Nutrition 1996;48:67-78.
3 – Mortensen SA, Rosenfeldt F, etal. The Effect of Coenzyme Q10 on Morbidity and Mortality in Chronic Heart Failure: Results From Q-SYMBIO: A Randomized Double-Blind Trial. JACC: Heart Failure 2014;2(6):641-649.
4 – Miller DW. The Government Grant System: Inhibitor of Truth and Innovation? Journal of Information Ethics 2007; Spring Issue: 59-69. Available here in pdf.
5 – Bergmann O, Bhardwaj RD, Bernard S, et al. Evidence for Cardiomyocyte Renewal in Humans. Science 2009;324:98-102.
6 – Kajstura J, Narasimman G, Ogorek B, et al. Myocyte Turnover in the Aging Human Heart. Circulation Research 2010;107:1374-1386.
7 – Nowbar AN, Mielewczik M, Karavassilis M, et al. Discrepancies in autologous bone marrow stem cell trials and enhancement of ejection fraction: weighted regression and meta-analysis. British Medical Journal 2014;348:g2688.
The post Statins Will Kill You appeared first on LewRockwell.
Leave a Reply